


EBOLA is Treatable.
EBOLA is Treatable.
per Dr. Jackie Stone, GP, Zimbabwe


Ebola is treatable.
Marburg virus is treatable.
As is SARS Cov-2.
—With similar regimens to those successfully employed by a few courageous doctors and other health practitioners in the US and elsewhere, using old, re-purposed drugs.
This is the testimony of Dr. Jackie Stone, General Practitioner, Zimbabwe. Like many practitioners elsewhere, she was hounded by her government for successfully treating Covid as she did. Her down-to-earth explanation here can teach us much about Ebola, Marburg, and Covid.
Pretty much everything she says here about Marburg virus applies equally to treatment of Ebola.
What follows is an interview —I’m not sure of the date. Cases of Marburg were reported in early 2023, so that is likely when this was posted. Video of the interview appears at the end of this post .
I believe part of the reason that this interview has not been more widely disseminated is because Dr. Stone, originally from South Africa, speaks with a pronounced South African accent which is hard to understand, presenting quite a barrier. Whoever originally posted the interview provided machine-transcribed subtitles with Dr. Stone’s slides. Unfortunately, the machine-generated “translations” are absurd in many places, especially when Dr. Stone uses medical terms,.
I have laboriously worked my way through her presentation and have rendered the best transcription of her words that I can —this is important stuff. In a few places I have shortened things, or changed a phrase or two, but I have tried in every instance to keep her original meaning intact. In places I have provided short definitions or clarifications of medical terms. I have also added a couple of footnotes.
I included this video as part of my earlier SUBSTACK post here:
https://haruhuani.substack.com/p/i-now-understand-the-covid-pandemic
You might wish to read or re-read that post as well, especially now that you can understand her! Transcribing this presentation, I have more thoughts about this Covid event, which I hope to discuss here on my SUBSTACK soon.
I think this presentation, delivered in Dr. Stone’s down to earth manner, will educate us all better about all three of these diseases, their treatment, and how exactly the treatments work
**************************************************************
The interview. Dr. Stone:
Is Marburg as dangerous as we’ve been told it is?
I don’t think Marburg is dangerous at all, and for a number of reasons.
First of all, it’s very difficult to contract it. So, you need fairly close contact with people around you. It’s not like Covid, being around in the street. You’re not going to have to mask everybody up. It’s going to be direct contacts that are going to have to be isolated, and those contacts will then be treated—and there are effective protocols that we know about.
One thing Covid teaches us is how to manage viruses that cause inflammation, thrombosis (clotting), and hemorrhage.
Marburg virus causes hemorrhagic fever. And everybody goes, “Oh, panic. Just like Ebola!” People hear Ebola, and they hear Marburg, and they go, “What are we going to do?” And they’re going to order panic and quarantine measures that have been suggested before.
That’s not true at all. We know that these treatments work because we watch them work.
Yesterday, Dr. Peter McCollough said, the world has concluded that we cannot vaccinate ourselves out of future outbreaks with untested, unsafe genetic vaccines, which is what I am understanding the WHO is planning to do with the new Marburg virus.
Our focus needs to be treatment, treatment, treatment, early treatment. We know it works.
The new hydroxychloroquine data shows unequivocally that hydroxychloroquine was working for Covid in March, 2020, and I’d even go back to another quote which we made then:
“Hit it hard, hit it early, and hit it with combination therapy.”
Here’s the fear porn for Marburg: “ Marburg causes hemorrhagic fever, up to 90% are going to die. A bat will inoculate you, with something that will inoculate YOU. Your lymphatic gets infected, and your lungs. Your liver, your spleen, your liver, your pancreas, your guts all fall apart. Lymphocytes collapse and kidney tubules stop functioning, and we have clots in our blood and then we die. “
No, that’s not what happens at all.
How does the virus kill the host? It doesn’t. It enters, it replicates, it assembles, and it is released.
What CAN kill people if not treated : Then you get a cytokine storm which causes huge inflammation. (My note: cytokine storm is your own body’s overreaction to the presence of the virus. It is your body’s out-of-control reaction, not the virus itself.) We know exactly how to manage cytokine storm, both before and after Covid, but we’re even better at it now. But if you are having an untreated cytokine storm, you get fever. and clotting, called thrombosis or hemagglutination. We have everything medically in place, meaning, we know how to stop the clotting. And, if you as a patient, don’t clot abnormally, then you don’t use up all the clotting factors in your blood—and you don’t bleed. If you control your cytokine storm you don’t get a fever, and if you control your clotting, you don’t bleed.
There is no such thing as hemorrhagic fever—if it is treated in the early stages.
Let’s go back to our friend, the cytokine storm. The cytokine storm is initiated as an inflammatory response to the virus. High levels of viral replication may initiate it. So—we shut down the virus.
Important—cytokine storm happens only in the vulnerable who are prone to inflammation. Dr. Sabine Hazen (US gastroenterologist physician and researcher} has beautifully demonstrated in her work that if there’s lots of bifida bacteria and you have a healthy gut, then you do not get a large cytokine storm.
What promotes a healthy microbiome--
Zinc, vitamin C, vitamin D.
We should all be on those three things every day. Anybody who is on those has nothing to fear from Marburg.
What kills people is not actually the virus, but is rather, cytokine storm, which causes direct organ injury.
People in Africa get lots of vitamin C in their diets because they eat a lot of tomatoes, they have a lot of vitamin D because they spend a great deal of time out in the sun. But African soils are low in Zinc.
So, the first thing we do to head off cytokine storm in Warburg patients in Africa is give patients zinc, even before giving them colchicine and over the counter antihistamines. But –important—a cytokine storm will only initiate in a vulnerable host who is prone to inflammation.
We don’t need to be scared of cytokine storms. They are controllable. Note we have not yet even discussed pharmaceuticals.
Because the best way to control cytokine storm is with a combination of silver and ivermectin.
We have known since 2014 (via in vitro studies then) that ivermectin treats Marburg.
Cytokine storm – thrombosis (clotting) –bleeding
A clot is actually the final thing that will kill a patient.
Cytokine storm causes clotting of the blood throughout the body. The way you clot, is your body releases what are called “clotting factors,” in your blood, that facilitate clotting. What happens when you use up all your clotting factors? You bleed.
With Marburg, we are talking Day 20 into the illness. We are three weeks in now! We’ve had lots of time to treat this. This isn’t happening in two days. By then we’ve gone through the viral replication phase, we’ve gone through a cytokine storm phase, and we’ve gone through thrombosis (clotting phase of the cytokine storm).
At about this time, a lab called the D-dimer goes up, and three days later, the patient bleeds.
We’ve got three weeks to treat it.
But it is when the platelets drop (because the clotting factors are all used up) that’s when we start to see the terribly, terribly scary picture, because the patient starts to bleed through their mucous membranes or under their skin.
So they show us picture of subconjunctival hemorrhages where you bleed into your eyes, and you’re vomiting and blood is coming out of you,
And that is happening because you haven’t treated it.
Just like malaria. If you don’t treat it, you’re going to end up in the ICU and you might die.
Just like Ebola, just like Covid, if you are untreated and you progress to severe disease, you are likely to die.
The whole point of management in Africa is that we treat early so that we don’t end up with a patient in the hospital because we don’t have very many hospitals.
Treatment.
Let’s go back.
How does a virus kill the host?
If we can stop viral entry into cell, stop viral replication inside cells, viral assembly and viral release, that’s a start. Then we won’t even get to cytokine storm, clotting, bleeding, and all the rest.
Both Marburg and Ebola are filoviruses, which means that they are squiggly little viruses. They are kind of squiggly viruses with lots of glycoproteins (combination of a protein with a sugar molecule) which would otherwise be spikes.
Interestingly, they are trimeric (three-pronged) proteins, which are very like a spike. And they behave exactly like the spike in that they use it to attach to a receptor in order to enter the cell.
At the point where the virus is entering the cell, if you have coated those glycoproteins on the virus with silver and ivermectin, then the virus can’t enter the cell. So now it hasn’t even got past level one.
If the virus does manage to enter the cell, it enters into something called an endosome, In the endosome, it hasn’t actually entered the cell because it hasn’t gone through the membrane. It’s not in the cytoplasm. In that endosome there is a lot of acid. The acid in the endosome will break down the virus and allow the RNA in the virus to release.
Two drugs stop this acidification and viral release in the endosome: hydroxychloroquine and azithromycin.
This is Dr. Zeb Zelenko’s protocol: hydroxychloroquine, azithromycin, and zinc.
At this point, with this treatment, the virus can’t get into the cell, or if it can, it can do so only in small numbers.
So let’s suppose that at this point we haven’t given hydroxychloroquine (because… “it does not work, “ …which we know it does), and we haven’t given azithromycin, and the virus has progressed .
Azithromycin has very powerful antiviral activity and this is one of them.
At this point, untreated, the virus fuses with the cell membrane and it puts its little piece of RNA into the cytoplasm. Now we have virus wandering around in the cytoplasm, thinking, “now I need to make proteins and more virus so that I can reproduce.” Here it goes along in the cytoplasm in a complex called a ribosome.
Doxycycline takes out the ribosome so the virus can’t make these proteins.
But—there is another complex here in the cytoplasm as well, an enzyme, called RNA-dependent-RNA-polymerase protein –long complicated word-- but all it is, is a photocopy machine. It’s making more and more copies of the virus.
That enzyme will be suppressed by high levels of zinc. And it will be suppressed by all the zinc ionophores which Zelenko mentions –hydroxychloroquine, chloroquine, doxycycline, ivermectin, quercetin.
(An IONOPHORE is a substance which helps a molecule like zinc to get past the cell membrane and thus get into the cell.)
We have already got pretty good treatment here, and we haven’t even got to the stage of just stopping the virus! It can’t make more copies of itself because hydroxychloroquine, chloroquine, ivermectin have stopped that.
It’s pretty much been stopped on four different fronts, which is why we use triple- and quadruple-therapy.
At this point you shouldn’t even get a cytokine storm.
It’s not hard.
So—what do we do at a viral level?
Under an electron microscope you will notice that Marburg has one long spikey RNA in it. Marburg has two curves, or folds, Ebola has one curve. Both viruses are covered all over their surfaces with spike-y glycoproteins. A glycoprotein is a spike. You’ve basically got spikes. I think this spike-y protein is GP-140. HIV spike-y protein is GP-120.
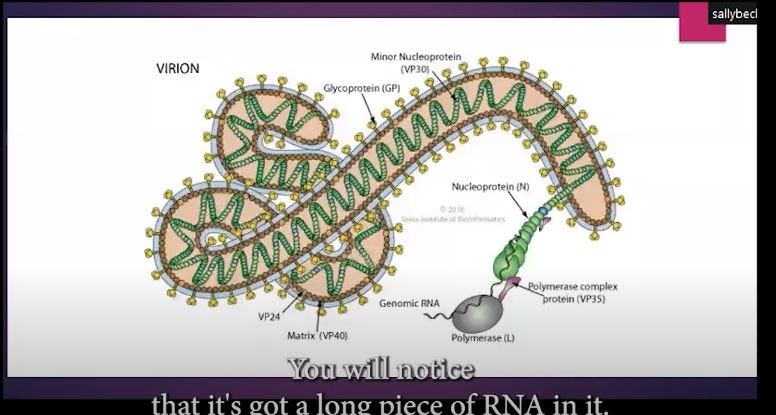
Here is an electron microscope view of an Ebola in the bloodstream (note round red blood cells surrounding the virus) , nice, long, stringy. Both Marburg and Ebola viruses are filoviruses.

You have to understand these diseases to treat them. These are not infections of the gut that make people vomit and pass blood. These are JUST LIKE COVID. They’re infections of the bloodstream and the endothelium. (Endothelium is the thin layer of cells that lines the interior walls of blood vessels.)
So these are the pictures that the WHO will show you, of people dying, feverish, with blood coming out of every orifice
And by the time you’ve got to this stage, you should have treated them…by the time they’ve gotten to this stage, you should have treated them two weeks before!
Let’s look at Covid.
WE HAVE TO UNDERSTAND THAT ALL OF THESE DISEASES — EBOLA, COVID, AND MARBURG —ARE DISEASES OF THE BLOOD AND OF THE MICROVASCULATURE (small blood vessels.)
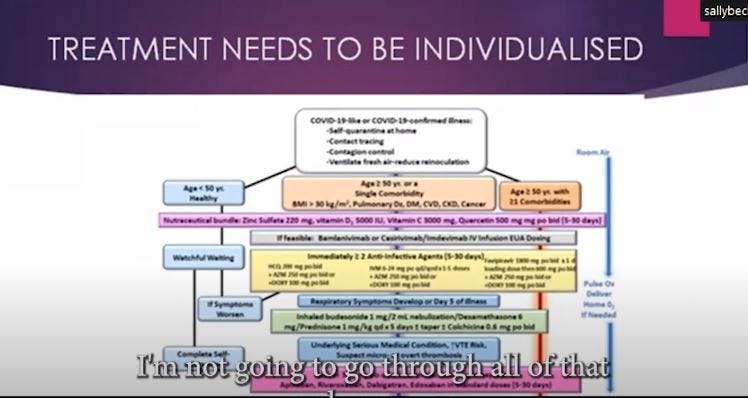
To treat these, you first need to risk-stratify your patients.
1. Young healthy patients: fill them full of Vitamin D, get them eating well, probably can also have Vitamin C and zinc.
2. If you’re a smoking hypertensive with three previous heart attacks, you need to go down to maximum treatment at all stages.
(GRAPHIC—I can’t read this chart below very well, but I think it looks a lot like Dr. Peter McCollough’s protocol. You can find that on his website--Haru.)
Sequenced multidrug therapies have been effectively used in Zimbabwe since 2020. I think we probably got it right in about 2021. The result was, we call it
THE SIDDz PROTOCOL:
SILVER
IVERMECTIN
VITAMIN D3
DOXYCYCLINE
ZINC
The result for Covid can be seen on the graph, below.

GRAPH:
In Nigeria (BLUE LINE), they gave ivermectin, Vitamin C and zinc but not doxycycline. Patients got better in 7 to 8 days. Malawi and Mali (ORANGE, GREEN lines)—they gave ivermectin, doxycycline, zinc, and patients were better in those countries in 24 hours —they never did require oxygen to be administered.
WHO, grey line: Remdesivir, Alluvia*. Enoxaparin (blood thinner), azithromycin, vitamin D, zinc sulphate. The patients’ oxygen never really did get completely better even after 10 days.
All the proof of the pudding is in the eating. We need results-based protocols, so I’m going to show quite a few slides without going into things in too much detail. I just want to reiterate:
Ebola uses the same replication mechanism as SARS Cov-2.
So does Marburg.
We know how to switch it off now.
The Drugs
Stage 1: Drugs to Stop Viral Replication.
Fusion Inhibitors coat the virus keep it outside the cell: Nano Silver, Ivermectin
RNA polymerase inhibitors keep the virus from making copies of itself: Zinc, Zinc ionophores (hydroxychloroquine, Chloroquine, ivermectin, quercetin), Ivermectin, Ionic Silver
Ivermectin and doxycycline were found to be the most effective here against Covid. We might find that a different combination works with this. But if we don’t know, we won’t try.
RNA Helicase inhibitors also stop lots of copies: Ivermectin, silver
ZINC: If there’s lots of zinc in the cell, there’s no RNA polymerase. This virus can’t replicate. You’ve taken it down.
Most of these drugs are available over the counter in Africa. If the patients are being told to get a vaccination, OR they can go to their friendly local traditional healer and pharmacist, and get medications that they know will work, I can tell you which one they’re more likely to go for.
Stage 2: systemic spread phase.
We also stop that with all the antiviral drugs, above, that I have just talked about .
A Few Additional Notes
The viral glycoprotein— (the tiny squiggly filaments along the length of Marburg and Ebola, and the spike protein on Covid) —we can approach it. The viral glycoproteins in Ebola, Marburg, and SARS Cov-2 are all basically the same. They’re like a small fishing hook. They cause the blood to coagulate. So it’s not actually very scary at all.
Oh, but people have said, the glycoproteins of SARS Cov-2 are 2 to 5 nanometers in size rather than 10 nanometers in size. It doesn’t matter. We just use a 2 to 5 nanometers in size silver nanoparticle to coat the glycoprotein. We know that cytokines are heavily suppressed by silver. Look—you.ve got 6-fold suppression of IL-6 and TNF-alpha (these are molecules that the body releases to cause inflammation ) , both of which cause the cytokine storm. Dexamethasone (steroid which was used in the US after much prodding of the CDC by a few courageous doctors) caused a 20% decrease in inflammation.
Old, simple drugs. But the whole world went crazy everywhere.
So, without going too much further here, I’m just going to go through one thing more about Africa. Let’s talk about some real-world evidence in Sierra Leone. Ebola—“the world’s coming to a grinding end. We’re all going to die. Mortality 40 to 50%. “
In Sierra Leone, where Ebola actually is, there was a 21.7% mortality rate. They halved the world mortality rate with silver alone. There is a trained chemist in African named Alpha Kanu, who was able to get a lot of silver into Sierra Leone. The FDA did whatever was in their power to stop it. The silver landed in Sierra Leone, and we’re not too sure what happened after that, although the president, Ernest Bai Koroma, got into the tussle with the bureaucrats to say, you cannot stop this from coming here.
If we look at ivermectin, we know that it works in Marburg. It is a completely safe drug. There is no reason not to use it. What’s the worst thing that’s going to happen? We’re going to have a parasite-free population. And we know for sure that a side effect from excess silver (argyria—skin turns blue) does not affect dark skinned patients.
Any time that anybody says to take silver you will be warned that your skin will turn blue. You would need to take ten grams of it, --you basically need to take about 20.000 doses of it-- to turn blue. And if you have dark skin all that will happen is, your skin will turn slightly darker. You would need to take it for about 10 years to take 10 grams, if you’re taking it in a colloidal or (nonabsorbable ? I could not hear this-- Haru) form. You couldn’t take it in a day, or if you did it would just pass through you, you would excrete it
If we’re looking at economic collapse in Africa, which will happen if we go into quarantine lockdown, and we wait for a new vaccine that is completely untested-- we already know from the Kenyan vaccination in 2014, where they vaccinated everybody, where they had HCG put into the injections as well as tetanus vaccine and they got a 40% infertility rate after that—people in Africa are not, I don’t think, going to particularly want any more vaccines in Africa where we don’t know what’s in them, particularly when we know that we have multiple ways that we can treat this virus.
I didn’t even get to how you can stop the clotting phase—aspirin. Some of the pharmaceutical like Xarelto, enoxaparin, or some of the naturals like nattokinase or seropeptase. And all of those things are available here.
Incidentally, for dengue in South America and Asia, popo leaf extract, in the end stages, saves huge amounts of people. (I am pretty sure she is meaning PAPAYA LEAF extract: see video, at the end of this post.**) There are several papers which will show that popo leaf brings the patient’s platelets levels up each day. In November of this year we posted a protocol: silver, ivermectin, doxycycline (?for dengue? --Haru).
Also incidentally, doxycycline given to Ebola rats results in a drop in the death rate from 90% to 40%, so there is a 50% drop in mortality with doxycycline alone, in rats. If we add silver, there’s another 50% decrease in mortality.
Doxycycline is called a broad-spectrum antibiotic but it is more properly called a broad spectrum anti-microbial. In order for a piece of genetic material to make a protein it has to go through a ribosome. Doxycycline blocks the ribosome. So if you’re a virus with a piece of genetic material, doxycycline won’t let you make a protein out of that piece of genetic material. If you’re a bacteria with a piece of genetic material, doxycycline won’t let you make proteins out of it. If you’re a malaria parasite, you’ll have the same problem. At the very basic, right down at the bottom basic level, doxycycline shuts down protein from genetic material. Doxycycline is also a zinc ionophore, which means it gets a lot of zinc into the cell.
When we remember that the ribosome is essentially a photocopying machine, that makes more and more RNA, and that the ribosome is inhibited by zinc, and that doxycycline puts lots of zinc into cells—doxycycline is a bit like a shotgun, where something like ceftriaxone (Rocephin) is more like a sniper rifle. You’re going to shoot meningococcus bacteria, meningococcus, with your sniper. If you shoot meningococcus with doxycycline, everything dies. Apart from the patient, usually, which is handy.
You see, we’ve got to get away from this labeling of all drugs. Ivermectin is labelled as an antiparasitic. But ivermectin has been known as an antiviral, as a secondary use, since 2010 or 2014. But it costs so much money to relabel it with the pharmaceutical companies (by this, I think she means that it is expensive and time-consuming to go through the entire regulatory process for each newfound use —Haru) , that it’s most up to say, right, we know it’s safe, we know it’s been through all the safety trials, we know it works, so we will use it as an antiviral. I use doxycycline extensively in malaria (which is caused by a parasite, not either a virus OR a bacterium) patients and it’s an antibiotic. But it’s on every protocol, to be used in combination with other medications, as an anti-malarial.
One thing Covid (authorities) seem to have tried to do is to say, for example, a certain drug is an antiparasitic, you may not use it for anything else. Well, that’s just the most bizarre way of thinking. If you understand the mechanism of action of a drug, if the drug is going to shut down the production of proteins from RNA, like doxycycline does, then it will work against viruses, bacteria, fungi, and cancer. (Because they all have to produce proteins! –Haru) Doxycycline and Vitamin C together shut down the production of proteins from mRNA, which is how cancer replicates.
So there’s a massive push against a lot of these drugs for a lot of reasons, because the cancer industry, the infectious disease industry, the vaccine industry, do not want stuff that is going to cost only $30, $40 for a whole course of treatment, AND keep the patient out of the hospital, AND that is widely available, particularly all over this country (Zimbabwe).
I guess the message is that the only thing to fear is fear itself. Marburg virus is a lot less infectious than Covid was. We have had a little pilot project where we set up a specific preventive protocol with older immune boosters, vitamin C, vitamin D, zinc. It included n-acetyl cysteine (NAC), which gives you a lot of sulfur and is an anti-oxidant that will stop cytokine storm. It included silver, ivermectin, doxycycline, and it included papaya leaf. And on the 11th of January this year, 2023, (Covid I think—mumbled) Uganda mysteriously vanished, due to the WHO’s “brilliant “containment measures in Uganda this year.
Our interest, here in Zimbabwe, and I think I may have said this on this recording, is that every time (some agency I think—I could not make it out) puts out that , “there is Ebola, or Marburg, in Equatorial Guinea”, every tourist cancels their flight to Africa, and it decimates our tourist industry, which it pretty much did. It collapsed over Covid. So, we have a very strong and vested interest, in countries that have a lot of tourism, and where there’s a lot of conservation of endangered species, that the tourists continue to come out. And this kind of fear-mongering nonsense, for want of a better word, will collapse our tourism industry. And it’s nonsense. It’s not a tiny transmittable virus (she is referring to the fact that both Marburg and Ebola require direct bodily contact in order to transmit) , and we know how to treat it. It’s not this big boogey monster bleeding out your eyes, ears and nose and there’s nothing anybody can do –as WHO and the rest of the world paint it.
You know, 400 children with HIV die in this country, Zimbabwe, every single month from TB as a result of poorly-controlled HIV. They die from poor access to drugs, and because of poor access to HIV services. We can thank lockdowns and economic disasters that resulted from those lockdowns, for those deaths. So not only are they neglected because the money is being spent on Covid vaccines. We haven’t had a single death from Covid. Marburg is so far away, it’s not even funny. And yet everybody’s getting hysterical and putting all their money into vaccinating against something where you’ve got to vaccinate 46,000,000 children to prevent one death.
In 2021 alone, we added 3,000,000 people to our extreme poor because of lockdowns, in a country of 14,000,000 people. So we’ve got malnutrition on top of that.
There are much bigger priorities than four cases of Marburg that’s going to shut down our tourist industry even further and put another million into the extreme poor.
Recently, when we had our so-called measles outbreak, only 2 died in hospital, which suggests that the rest died in abject poverty in the middle of nowhere. So they rolled out a measles vaccine and gave it to all the healthy children in Harare (capital of Zimbabwe) and did nothing about the starving in rural areas.
It makes absolutely no sense to me what’s going on. At least somebody is making a lot of money out of vaccines. All the vaccines have another agenda, which, as you know, Kenya thinks is de-population.
(The interviewer finishes by noting that in the west, access to good food and clean water, and that Bill Gates started his philanthropic journey by wanting everyone to have access to clean water. But that has changed and we don’t really know why. Dr Stone’s response:)
My last slide. Have a little read of what I think Bill Gates is interested in, in Africa:
And unfortunately, all us pesky Africans won’t die and get off the continent. So we need to be injected and sterilized so that they can turn the whole place into a line for their lithium, for their gold and their platinum, for their art of artificial intelligences.
The Congo could grow enough food for the world with its rainfall. So, Africa is not for little old Africa. Africa needs to be kept in its place with donations from WHO, so that we continually believe that we are inferior and that we need them.
END OF INTERVIEW.
Here is a link to the actual video:
https://drive.google.com/file/d/1k12q-HdHDPkzL8nmhFLvAb_zmql718j3/view
(I originally had to download Dr. Stone’s presentation from Google Drive to view it. I don’t know who conducted the interview. Perhaps someone in the comments below will let me know. )
*******************************************************
Dr. Stone’s BIO from her website:
Dr Jackie Stone is a practicing doctor with over thirty years of experience in the medical profession. She achieved a Bachelor of Medicine and Bachelor of Surgery, and a Bachelor of Science in Medical Biochemistry with Honors from the University of Cape Town, a Diploma in Aviation Medicine from King’s College London, and holds a Membership of the Royal Colleges of Physicians in the United Kingdom. Furthermore, Dr Jackie spent twelve years practicing Aviation Medicine at Emirates Airlines and worked in Dubai during the SARS pandemic in 2003 and 2004 and is an inaugural fellow at the Australasian College of Aerospace Medicine.
*(Alluvia is a combination of two newish antiviral medications, lopinavir and ritonavir. )
“There is currently no strong evidence for the efficacy of lopinavir/ritonavir in the treatment of COVID-19. Overall, the limited studies identified were subject to methodological flaws.
A two-week course costs approximately £140 (USD 170) in the UK11, and approximately £6.50 (USD 8) in certain low- and middle-income countries under pooled patent agreements13.” — Centre for Evidence-Based Medicine)
**Video: Papaya Leaf for low platelets in Dengue
https://www.youtube.com/watch?v=kweaQEzRFK

I see that there *were* six videos on YT by Dr. Stone discussing the reduction of covid using IVM. Those videos do not exist anymore, of course.
In Discussion With - Dr Jackie Stone
MedicalUpdateOnline
6 videos 1,227 views Last updated on Apr 23, 2021
"The use of ivermectin for prophylaxis and treatment of covid-19 in Zimbabwe has resulted in a 10-fold reduction in mortality. IMI interviewed Dr Jackie Stone, a family medicine physician based in Harare, Zimbabwe to find out more."
Thank you for transcribing that lengthy message.